Yesterday we explained you what Herd Immunity means and how it works, today we will take the discussion further to determine whether it is effective and can be recommended in the current context.
COVID-19 currently does not have a cure or a vaccine. Lockdown is the only strategy that appears to be working. Could implementing policies that encourages herd immunity be used to accelerate immunity in the population without the need for a vaccine?
- INFECTIVITY
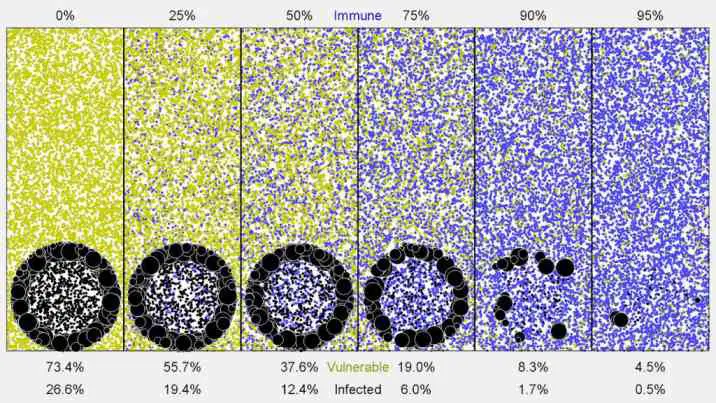
For the strategy to work we need to know a few things about the virus. How infective is it? In one of our earliest blogs we discussed infectivity at length and determined that the R0 (infectivity) may be between 2 and 3. This means each person with the virus can infect around 2-3 people at a time. Whilst this is not as high as Mumps (10-12) it is much higher than the common flu. The higher the R0 the more people that need to be immunised before herd immunity is achieved. For COVID it is estimated that 70% of the population need to be infected.
This is based off our current testing. Due to shortages in testing kits, only testing those that have a high likelihood of being infected and poorly organised testing infrastructure in some countries, we are likely underestimating. The number of people infected may be much higher as we are missing those that are asymptomatic but still have the disease and are still passing the disease on.
- MORTALITY
Secondly, we need to know the mortality from COVID-19. Early estimates of mortality were as high as 10%, as we had little data on how many people were truly infected, but as the number of infected cases rose, and testing amongst the infected and symptomatic population rose, a more accurate mortality has been found to be around 1%. There is a risk we may still be underestimating the true mortality, as some cities have noted a spike in cardiac deaths, and some evidence supports possible cardiac damage due to COVID. But from the data we have, we know its mortality is lower than MERS (34%) and SARS (10%) but more than influenza (0.1%).
estimates of the COVID-19 case fatality rate
Whilst we have some data on who is likely to suffer from severe COVID symptoms (elderly, immunocompromised, people with heart or lung problems) we still cannot accurately determine who will get severe COVID in the “low risk” population. Simply because someone is young and healthy does not mean they will not die from COVID.
- LENGTH OF IMMUNITY
Third we need to know how long this immunity will last. Similar coronaviruses responsible for the common cold usually create immunity that lasts for a few months, which is why we often get the cold repeatedly. A virus is also very prone to mutations that can change the structure and functions of its proteins, proteins responsible for tagging, latching on to and entering cells. If the structure of these proteins changes enough, then our antibodies will not be able to bind on, and new types of antibodies will have to be made with a slightly different structure. This effectively means our bodies have to start from step 1 again to create immunity, and we have to make new vaccines. This mutation rate is why we have to make new vaccines every season for the flu.
- LONG TERM COMPLICATIONS
Finally, we need to know if there are any long-term implications from a viral infection. Again, this is something we do not know yet, as the virus has only been around for a few months. There may be implications for the cardiovascular system, long term breathing problems or more. And even if the complication rate appears relatively low (say, 1%), if millions of people are allowed to get infected, by definitions thousands or tens of thousands of people will have these complications, complications that can lead to issues later in life or an early death.
CONCLUSION
So, is herd immunity a viable strategy for COVID? Without a safe vaccine the general consensus appears to be no.
We don’t know how infective the virus really is or how many people it has infected
A 1% death rate is still very high. This means for every 100 people to be infected; one will die. This would mean hundreds of thousands of people dead in a country with a population over 10 million. It is unacceptably high.
If the death rate is 1%, then hospitalisation rate is likely higher. Almost all countries do not have capacity to have 1% of the population in hospital. Overwhelming the healthcare system will lead to poorer care, and worse care for those who do not have COVID. Leading to more people coming to serious harm or dying as a result of poor healthcare, not because of COVID.
We don’t know the long-term effects of COVID. By purposefully infecting people instead of waiting for a vaccine we may be causing unnecessary damage to a person’s health that only becomes apparent later in life. But this is speculation as we do not currently know if COVID has long term effects,
We don’t know if all of the risks above will amount to anything. The immunity may not last long enough, leading to another spike in infections and mortality.
Mass vaccination appears to be the safest strategy. And though human clinical trials have started on a number of vaccines, we are still months away from deployment. Until then we should not come out of lockdown prematurely, not until we have received an unbiased assessment from public health officials that states it is safe.